








Breast Augmentation (Implants)
Conveniently located to serve the areas of Dallas, TX

Breast augmentation, also known as breast enhancement, is a popular cosmetic procedure designed to enhance the size and shape of a woman’s breasts. It is a sought-after surgery because many women desire larger, fuller breasts for various reasons. Whether it’s to enhance their overall appearance, restore breast volume lost after weight loss or pregnancy, correct asymmetry, or improve self-confidence, breast augmentation can help women achieve their aesthetic goals.
At USA Plastic Surgery in Dallas, Dr. Steven J. White offers personalized breast augmentation procedures to help patients achieve their desired breast size and shape. To learn more about how breast augmentation can benefit you personally, call USA Plastic Surgery at (214) 833-6751 for a consultation with Dr. White.
About Breast Implants
Breast augmentation sounds simple, actually deceptively simple. We are going to make the breast larger by putting an implant in. But it’s actually much more complicated than most people realize because there are a lot of variables that need to come into consideration.
Above or Below the Muscle?
We can go either above or below the muscle. (1) And I think it’s generally good to go under the muscle because it looks better. It feels better. It’s more natural. It’s easier to read a mammogram. There’s more support.
Which Incision is Best for Breast Augmentation?
And we have four options for incision. We can go under the arm. We can go under the nipple. We can go through the belly button or under the fold. (2) And we prefer to go under the fold because it’s the furthest away from the nerves with the least chance of numbness. It’s the most direct approach to see what we’re doing so that we can have the most control over what we’re doing. And then if we ever were to need another surgery, that’s where we would tend to go. Plus, I think it’s the least noticeable of all the incisions.
Round or Teardrop? Smooth or Textured?
We’ve talked about the type of implants, whether they are saline or silicone, and we’ll address that a little more. The shape of the implants, either the round or the teardrop. The concept with the teardrop is that it has a certain shape to it and perhaps not as full on the top. But what we find is that because it has a defined shape, if it rotates one way or the other, it tends to look somewhat goofy, and it would require another surgery in order to fix that. And most people prefer more fullness on the top, so that’s why the round tends to be more popular, because no matter how you spin it, it’s still round. Now just because the implant is round doesn’t mean that you’re going to have a round ball on your chest. The idea is you can get a beautiful result with any type of implant. The secret is we have to match the implant to your tissues.
And the texture of the implant, either smooth or textured. We tend to prefer the smooth implants because they move about a little bit more freely and they’re less likely to ripple.
Before and After Photos





Contents
- 1 About Breast Implants
- 2 Before and After Photos
- 3 Elegant Precision™ No Bruise* Breast Augmentation / Implants
- 4 Optimized Rapid Recovery
- 5 Saline vs. Silicone Implants
- 6 Before & After Pictures: Patient 1
- 7 Before & After Pictures: Patient 2
- 8 Before & After Pictures: Patient 3
- 9 Breast Implant Sizers
- 10 Implant Profiles
- 11 Creating Cleavage
- 12 Breast Augmentation: Risks
- 12.1 Capsular Contracture
- 12.2 Implant Rupture
- 12.3 Infection
- 12.4 Numbness
- 12.5 Exposure or Extrusion
- 12.6 Wrinkling
- 12.7 Asymmetry
- 12.8 Subpectoral Placement
- 12.9 Hematoma
- 12.10 Interference with Breastfeeding
- 12.11 Calcium Deposits
- 12.12 Breast Cancer or Interference with Mammography
- 12.13 Symmastia
- 12.14 Breast Implants Stretch Marks (Striae) and Inverted Nipples
- 12.15 Immune Disorders and Presence of Silicone Rubber
- 13 Medications – Why Muscle Relaxers Reduce Pain After Breast Implant Surgery
- 14 Post Operative Instructions After Breast Implant Surgery
- 15 As you Heal after Breast Enlargement Surgery
- 16 Cost of Breast Augmentation in Dallas
- 17 References
Steven J White MD
USA Plastic Surgery – Dallas, Texas
Elegant Precision™ No Bruise* Breast Augmentation / Implants
(*No Bruise >95% Breast Implants / Enlargement Patients)
Read Transcript of Dr. White’s Video:
Optimized Rapid Recovery
The Optimized Rapid Recovery Breast Augmentation enables you to have in most cases, a very quick and very easy recovery. In fact, a lot of patients go back to work the next day. I think this is not the out-to-dinner breast augmentation, but instead the out-to-lunch the next day.
7-Step Optimized Rapid Recovery Breast Augmentation
There are 7 steps with the Optimized Rapid Recovery Breast Augmentation.
Step 1: We want to listen to you. I want to understand what it is that you would like to achieve.
Step 2: We need to listen to your body and we’ll take some measurements, not only of the chest wall, but also the breast. And there are a number of precise measurements. This needs to be customized to fit you in order to achieve the prettiest pair of breasts for your body.
Step 3 is to teach you, because the more you know, the better you do. Regarding the size, this is one of the hardest things for most patients to kind of understand.
It really is a leap of faith. You have to trust me on this. The number one reason to redo breast augmentation is to change the size. Usually, to go a little bigger, sometimes to go smaller. But I think the problem is that both the patient and the surgeons go about it all wrong. A lot of surgeons will have you trying a bunch of implants in a bra, and that’s a great way to sell you surgery and get you excited about surgery, but it’s also a way to get you the wrong size. And it doesn’t really matter what the implant looks like under your bra. What really matters is what does it look like under your skin? And the only way you can figure that out is in surgery. So, what I want to do is I want to listen to your body, and very often we’ll use sizers, and that allows us to get just the right size for you.
And what I will often do is fill it (if saline) to the point it looks abnormal, back off to the point it looks natural, and then listen to that little voice where you tell me what size you would prefer to be. Now I’m not talking A, B, C cup. What I’m talking about is “just right”, “the largest size that still looks natural”, “as large as possible”, or “small, small”. So, we want to titrate it (or adjust it) in a way that fits your body, that matches your tissues, that also matches your tissues with your wishes. So, step 3 is patient education.
Steps 4, 5, and 6 we do in the operating room.
Step 4: We make the pocket. And I make the pocket under the muscle. There’s two ways to do this, either bluntly or precisely. I vote precisely. Takes me a little longer, but I use a little electric pencil and I go and make a space under the muscle to create just the right size pocket.
I keep it snug on the sides and only open it just as much as I need to at the end, and that helps me avoid injury to the nerves on the side. It also helps me to snug the breast up so that when you lay down, they don’t go places you don’t want to and fall off to the side. And then we release the muscle a little bit on the inside. And after the pocket is made, typically I’ll see little blood vessels and I’ll zap them before I go through them. And in most cases, we have no bleeding, or perhaps maybe a teaspoon of blood, which means most patients have little and most patients have no bruising whatsoever. It is possible you may have some bruising, but for the vast majority of patients, they have no bruising. They’re off pain pills in 24 hours.
Step 5: Match the implant to the tissues. And this is really the most time-consuming part of the operation, because this is the customization. This is how I can get the prettiest breasts for your body. And one of the things I like to do during surgery is while you’re asleep, I will sit you up, and then I will compare between both breasts to make sure they’re in the right position, to make sure that they’re the right size, and then to look at the shape.
And sometimes we’ll do step 6 and that is sculpting of the breast to reshape the breast over the top of the implant. And then finally, step 7 is the postoperative care. And we’ll go into that in a little bit more detail.
Saline vs. Silicone Implants
The very first implants were placed in 1962, and they were silicone gel implants. (3) They were placed underneath the breast on top of the muscle. And the problem with the early gel implants, where the outer shell of all implants is silicone, the inner gel was really watery and the outer shell was kind of leaky. So, the first-generation breast implants would tend to leak, and the body reacted with scar tissue.
And the body normally forms the scar tissue around the implant that’s called a capsule. Then you want a very thin, soft, supple, not thick, tight, hard scar around the implant. If it’s thick, tight and hard, it’s called a contracture. That’s what we want to avoid.
And in order to avoid the contracture, that’s why they developed saline implants, was because if it leaked out, your body didn’t respond to saline because two thirds of your body is saline. They also learned in studying what led to these contractures was that if you went under the muscle, you had a much better blood supply and a lot less chance of a contracture.
At first, they put textures on the implants, and the thought was that it would break up the scar tissue. And what they discovered was if you could avoid infection, avoid bleeding, go under the muscle, do precise surgery, and then do range of motion exercises to keep it moving afterwards, it really didn’t matter whether it was textured or smooth. And the textured implants would tend to be a little thicker and a little bit more likely to ripple.
Cohesive Silicone Gel Implants
The current gel implants are much, much better. And in fact, I now love them. But worldwide, over 90% of implants placed are silicone gel implants. The outer shell is more solid. The inner gel is more cohesive. If you slice it and squeeze, it’s almost like a boomerang. It’ll go and then it’ll come back. Most people feel that a gel implant feels a little more natural than a saline implant. They’re a little bit lighter. So, if someone is pretty athletic and likes to run, they have a little less weight.
But one of the biggest advantages of the gel implant is they’re much less likely to ripple. Saline is a very good implant, although in some cases, the saline may tend to ripple. The question is when does that really matter? I think if you put an implant under a D cup breast, it probably doesn’t matter much because you have a lot of tissue to cover the top of the implant. But if you’re placing an implant under an A cup or a B cup breast, then there’s very little tissue to cover the implant and then you’re going to feel more implant. And if there’s a difference in the implants, it’s going to be more noticeable.
If you should develop rippling, then that’s something that you would be more apt to feel and possibly even see. So, I think that’s a pretty good understanding of what the difference between the saline and the silicone gel implants are.
Before & After Pictures: Patient 1
Let’s look at a few pictures from the plastic surgery book. For breast augmentation, the first patient I think is very interesting because she has very little breast tissue. And if we just took five measurements, based upon her breasts, we would end up putting in an implant that is too small for her tissues. So we have to take into consideration, not just the width of her breast but also the width of her chest wall. And when we do that, we want to match the implant to her chest wall that then expands her breast and it creates the curves on the side, and I think that creates a very natural contour for her. I saw her and I thought she has beautiful breasts to begin with. And she says, “yes, thank you. I love them, except I’d like to go bigger.” And I said, “but you look beautiful the way you are.” She says, “thanks, but I’d like to see you and raise you 20.” And I said, “okay.” So she starts with a very natural look and she just prefers to go bigger.
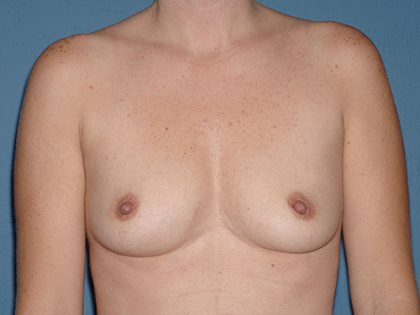
Before & After Pictures: Patient 2
This is a young model. Again, we can see how her breasts are not matching her chest wall. She has very little breast tissue. One areola on her right is a little bit bigger. The nipple is a little higher. Her fold is actually a little tight. And if you can see her bra mark, you can see where her fold should be. And so in this particular case, what I’ve done is I’ve lowered her fold, placed the implant in the right place, and matched across the top. And I think that’s a very nice result for her.
Before & After Pictures: Patient 3
And the last patient, I think she has very pretty breasts to begin with. She felt that she’d lost some volume over time and wanted to go a little larger to provide fullness, particularly in the upper pole. And again, as we can see, I think this is a very natural match across the top and overall size, and yet it still provides the additional fullness that she was looking for, particularly in the upper part of the breast.
Breast Implant Sizers
Let’s talk a little more about matching the implant to the tissues. Again, the goal is the prettiest pair of breasts for your body and we want to match the implant to your tissues. Now, there are some patients who have very tight skin and they want to go as big as possible. Well, their body’s not going to allow that. There are some patients whose tissue is perhaps a little bit looser that may not want to go too big. Again, you have to provide an implant that fills out the breast.
Implant Profiles
There are different profiles of the implants. There’s the low profile, the moderate profile and the high profile. And the low profile is kind of flat. That’s your baby bear. The moderate profile is your mama bear. And then your high profile is your papa bear. This is a fun part. What I want to show you is an example of the same amount of CCs displayed three different ways.
Now you’ll notice that the base diameter, the one on the right is wider than the one on the left. The higher the profile, the taller the implant. The one on the right we tend to not use, because I think it’s a little bit flat. We often use the moderate or the high profile.
Next, I want to show you the same base width with three different sizes. These implants differ by 75 CCs. So we start with the one on my right, that’s a low profile. The moderate profile is the same width, but it’s 75 CCs taller. Next, we go to the high profile, which again is another 75 CCs taller for this given base diameter implant.
First, we want to go with the size of your chest wall and match the implant to your chest wall, and then look at the laxity of the tissues and adjust the implant size based upon how loose the tissues are and also based upon what you hope to achieve.
Creating Cleavage
My goal is to create as much cleavage for you as we can and still look natural for your body. We like to achieve this by matching the implants to your tissues. Now, there is only a certain amount of cleavage that I can generate with your tissues. In other words, what I need to do is center the implant under your breast. If the nipples and the breast are a little more to the side, then what I need to do is place the implant and center it under your nipple and under your tissues provide more fullness on the side and that tends to bring the nipples more towards the middle and enhance the cleavage.
If the breasts are a little further apart and I place two implants very close together, it will actually take the nipples and push them to the side, and that would accentuate that look where the nipples would be pushed to the side. So again, I want to achieve as much cleavage as your body will allow, and yet still make it look natural. To maximize the cleavage, after surgery you can always do the miracle bra and that’s the click, click, click.
Breast Augmentation: Risks
The risk really comes into two basic categories. There’s a risk associated with the procedure itself, infection, bleeding, malposition, rupture, deflation, contracture, numbness, those type of things.
And then there’s a risk regarding the outcome. In other words, what does it look like? What does it feel like? Does it look natural? Does it fit their body? So, these are both considerations that we want to think about.
Capsular Contracture
The first would be capsular contracture. The capsule is the scar around the implant, and that’s normal. Anytime you put something into the body, the body forms a little layer of scar tissue around it, and we call it a capsule. What we prefer is a very thin, soft, supple, loose capsule,not thick, tight constricting. That’s a contracture.
What causes contractures? Infection, bleeding, lack of motion, on top of the muscle. Let’s go under the muscle, avoid the infection, avoid the bleeding, and then do the range of motion exercises.
If you keep the implant moving, that stretches out the capsule and prevents it from getting tight. If you never move it, it’s going to do a purse string-type effect and constrict down around the implant. This capsular contracture is very rare if you do precise dissection, avoid bleeding intraoperatively and postoperatively, avoid the infection, go under the muscle, and do the range of motion exercises. But it can still happen, and if it does, it can lead to tightness of the breast, firmness of the breast, malposition of the breast, and possibly even pain. And should you develop one capsular contracture, then you’re more apt to develop another. And it could be that if a patient developed this, that it could come to the point that they develop recurrent contractures and they may just want to take the implants out. That’s very rare, very unlikely, but it’s within the realm of possibility.
Implant Rupture
If a saline implant is ruptured, it’s pretty obvious. Some people would say it’s like a flat tire. You have a full breast and suddenly you have a deflation. Saline implant – saline is salt water, two-thirds of your body is salt water. Your body will just absorb it. And then you’ll probably give me a call pretty quickly and say, I think it’s a good idea if we can go have this exchanged.
If it’s a gel implant, silicone gel implant, it’s harder to detect a rupture. That’s why there’s a recommendation to get an MRI and periodically check the implant with an MRI to detect a silent rupture. In other words, you can’t see it, you can’t feel it, but you might see it on an MRI. And the recommendation would be that if it’s ruptured, that you would want to replace it.
Infection
Infection for breast augmentation is very rare, but that’s a serious problem. Should you develop an infected implant, this may require going back to the operating room, taking out the implant, washing it out, putting in a drain, putting you on six weeks of IV antibiotics. And it could require removing both implants, leaving them out for two months before replacing them. I am very, very diligent with sterile technique, and it’s also very important for you to be careful and to take the antibiotics as prescribed. Again, these are doctor’s orders, not doctor’s wishes.
Numbness

Loss of sensation of the skin or the nipples. Generally, this is minor and tends to come back over a period of several weeks and several months. Nerves are funny. It takes about two years for the sensation to come back. At that point, after two years, it’s as good as it gets.
The nerves start out under the arm and end up at the nipple. If we stay away from under the arm and stay away from the nipple, and by going under the fold, we’re further away from the nerves and less likely to have numbness. The nerves come from the side, and that’s one of the reasons why I keep the pocket snug on the side and only open it as much as I need to in order to find the right size implant for you.
Exposure or Extrusion
Exposure or extrusion of the implant. It’s possible for the wound to open or for the implant to fall out. Never seen one fall out yet, but it’s a possibility.
Wrinkling
Wrinkling or rippling of the implant. Again, this is more likely with a saline versus a gel. Very unlikely with a gel implant. The muscle runs along the lower ribs, the sternum, and up to the arm like this. This area over here is not covered by muscle, just covered by breast tissue and skin. So if you were to develop rippling, that’s the area that it would be most likely to see or feel.
Now there’s a distinction between rippling of the implant, and as you lean forward, the weight of the implant pulling against the capsule. If you’re pretty thin and you have very little tissue to cover the implant, as you lean forward, you may be able to see the weight of the implant pulling against the capsule. That’s not actually a ripple of the implant, that’s just the edge of the capsule that you’re seeing.
Asymmetry
Now, no two breasts are identical. For everyone, one side is a little different than the other. And again, the goal is to minimize the degree of asymmetry, but there’s an adjustment phase where they adjust to you and you adjust to them. At first, they ride high and then they slowly settle down. And we hope that they settle back down to where we have placed them during surgery in order to get the most natural result.
Subpectoral Placement
Subpectoral replacement of the implant. This says we start out under the muscle, and the objective is that we would stay under the muscle. It’s possible that it could flip up and come over the bottom of the muscle and get a double-bubble type effect that is extremely rare.
Hematoma
Hematoma. That’s bleeding around the implant, and that’s something we want to take great care to avoid. One of the reasons why I want to take my time during surgery is to do a precise dissection, and also to avoid not only bleeding during surgery, but also then postoperative bleeding. And I need your help on this. You have to play by the rules. You can’t go run, and jump, and lifting, things like that, because by the time you do, it’s too late.
Loss of Skin: Breast Tissue or Nipple
Loss of skin, breast tissue, or nipple. That’s extremely unlikely, but within the realm of possibility.
Interference with Breastfeeding
Interference with breastfeeding, that’s possible.
There are a number of women who have implants that breastfeed just fine. There are some women who don’t have implants, they can’t breastfeed. If you have implants, you may or may not be able to breastfeed. (4) But many patients who have implants are able to breastfeed just fine.
Calcium Deposits
Calcium deposits and the tissues around the implants. This is very unlikely. With a preoperative mammogram, if you have underlying calcification, then this can be followed over time in those cases, for which it makes sense to get a preoperative mammogram.
Breast Cancer or Interference with Mammography
Breast cancer. The studies show that implants do not cause breast cancer. Most patients who have implants that are subsequently diagnosed with cancer tend to present at the same stage as someone who did not have implants. There are special techniques used in a mammogram for a patient who has breast implants in place. It’s easier to read a mammogram if you’re behind the muscle, because you’re a little further away from the breast. But it’s always a little harder to read a mammogram if there’s an implant in place.
One of the reasons we go behind the muscle is it makes it easier to detect cancer on a mammogram, although it is still a little bit more difficult with an implant in place. They do the digital studies now, and they have a great deal of experience reading mammograms in patients who have implants in place.
Symmastia
Symmastia would be lack of cleavage, which would be like a mono-breast instead of two breasts, but one that crosses the midline. Again, that’s extremely unlikely. But if that were to be the case, that may require an additional procedure.
Breast Implants Stretch Marks (Striae) and Inverted Nipples
Stretch marks or striae. Again, this is very unlikely following breast augmentation, although patients will sometimes develop some stretch marks in their breasts just from gaining a few pounds or losing a few pounds. So, there are a few patients who may develop some stretch marks.
Also, the areola may enlarge somewhat if it’s stretched during breast augmentation.
Patients who have inverted nipples, this is something that’s often corrected by breast implants, because if the nipple is inverted and it’s able to come out on its own with a little bit of pressure, if you put an implant behind it, often it’s enough of a pressure to help correct that.
Immune Disorders and Presence of Silicone Rubber
Immune disorders. Breast implants are probably the most studied medical device in U.S. history. Since the FDA took the gel implants off the market in ’92, they’ve been studied extensively, and the studies have shown that they do not cause the underlying medical problems that they considered that perhaps they might have with rheumatoid arthritis and lupus and all of those connective tissue type things. And that’s why the FDA reapproved the silicone gel implants in the U.S. for routine use in 2006. Presence of silicone rubber. Again, all implants have a silicone solid shell, whether it’s a saline on the inside or a silicone gel on the inside. (1)
And the alternative is to do nothing.
The Brava device for nonsurgical enlargement of the breast. The idea was you put a large suction cup on your breast for external tissue expansion, and if you wore these really large domes for 12 hours a day for three months that perhaps this might grow your breasts just a little. It does grow just a little, but if it grows the breast, it might possibly grow breast cancer. And I think that’s one of the reasons why it has never taken off.
Medications – Why Muscle Relaxers Reduce Pain After Breast Implant Surgery
The medications are the same as I had discussed previously. The difference is I like to add a muscle relaxer for breast augmentation. We give you a dose during surgery and that helps relax the muscles. And then after that, we have you take one pill several times a day and wait about an hour after that, before you do the arm exercises. And that’s just a jumping Jack sitting still, and that helps stretch out the muscles.
Again, most of your pain is because the muscles are tight, and they’re being stretched. And so, if we can relax the muscles, that minimizes your pain and also allows the implants to settle.
Post Operative Instructions After Breast Implant Surgery
After surgery, you’ll go to the recovery room. And then when you feel comfortable, then we’ll have you go home. It is important to drink fluids. You must take your antibiotics. I’d like you to take your muscle relaxers, do your arm exercises. And I want you up walking in the halls or walking around the house.
At first, the implants are going to look kind of weird. It’s better if you just leave everything alone until you come to the office, and we will walk you through it the first time. So, try not to look. Just sponge bath for a while until I see you back in the office, because the first time you look at it, you’re going to kind of “wig out”. They’re going to look high. They’re going to look square. They’re going to look swollen in between and kind of wide apart. They’re going to look swollen on the side. It’ll look long to the nipple, short underneath.
Postop Bras – Why the Right Bra is Essential for the Best Breast Implants Results
We typically will put you in a flimsy bra early on until the breasts begin to settle into the position we’d like them to be in. At that point, we’ll switch you to the super-spiffy bra, and that gives you more support to help hold them in place, because we want to maximize the cleavage. So we want to keep them snug when you’re laying down, otherwise over time, as you’re laying down flat and sleeping at night, they may tend to stretch on the sides and you begin to lose a little cleavage. Also, we want a snug band underneath, because as time goes on, the breasts begin to droop over time. If you’re 80 or 90 years old, the breasts are not up here, they’re down here. So the idea I think for any woman is to maintain good support, particularly if we have implants in place. I think it’s helpful if you sleep on your back, at least for the first week, hopefully for the first couple of weeks, therefore you’re not putting any undue pressure on the implants.
Postop Orders – BEHAVE!
This is really important. Don’t do anything strenuous. Don’t do anything that causes bleeding. Running, jumping, lifting, anything like that. If you think that you shouldn’t do it, you’re right, you shouldn’t.
Bathing and Showering after Breast Enlargement Surgery
I prefer for you to just sponge bath for a short period of time until you come back to the office for us to take a look at you. It’s easier if we walk you through the operation and what you look like after surgery. If we can share that with you the first time, we can explain it. It makes much more sense.
You have steri-strips underneath. If it bleeds a little bit under the steri-strips, that’s totally normal. It may look a little “grungy,” I guess. But if you see a little discoloration under the steri-strip, don’t worry about it. They’re waterproof. We wait about two and a half, maybe three weeks before we take them off. And what you’ll find, we’ll show you with a mirror. Typically, it’s a very fine line incision.
Exposure to Sunlight and Driving after Breast Enlargement Surgery
Exposure to sunlight – Be sure you don’t get a sunburn. Actually, it’s very important not to get a sunburn before surgery. If the skin is burned and then we stretch it during surgery, that could lead to stretch marks, it could also impact upon your healing. So be sure and avoid a sunburn both before, as well as shortly after surgery.
Driving – Try not to drive when you’re taking narcotics, but most patients are off narcotics in the first 24 hours. And after that, if you feel like you’re okay, then I think it’s fine for you to drive.
Sexual activity is like sports and activities. That’s about a month. One thing I’ve noticed is there’s a big spike in both babies and engagements after breast augmentation. So, if you weren’t planning on having kids … just make sure you take precautions.
As you Heal after Breast Enlargement Surgery
Maybe two weeks after surgery, you begin to get super sensitivity of the nipples, and sometimes it gets real sensitive. And if that happens, it usually shows up a week or two after surgery, usually lasts for a week or two, and then slowly begins to fade away and often goes back to normal.
- Asymmetry – Again, both breasts are not identical before surgery. As they heal, again, you have to adjust to them, they have to adjust to you. And very often they go back to where we put them during surgery, which creates as much symmetry as I’m able to achieve with your body.
- Sloshing sensation – This is kind of fun. If you’re walking along, you may hear a sloshing. Don’t worry, other people don’t hear it. And what you’re hearing is air in the pocket around the implants. The body soaks up the air and that goes away.
- If you’re lucky, you’ll get what I call the “rice crispies.” And that is subcutaneous emphysema. That’s a little air in the tissues. And if you push on the skin, it feels like rice crispies. It’s not anything to worry about, but it’s kind of a fun thing if you can push on the skin, it’s like little tiny air bubbles.
- The skin’s sometimes a little shiny at first because of the stretching of the skin, and that tends to fade as time goes on.
Again, thank you so much. I’m very excited for you. This is a wonderful operation and a great deal of fun. Thank you.
Cost of Breast Augmentation in Dallas
The cost of your breast augmentation surgery will depend on your individual treatment plan. Following your comprehensive consultation with Dr. White, we will provide an accurate cost estimate. Call USA Plastic Surgery at (214) 833-6751 or contact us online to find out more.
References
- Fardo D, Sequeira Campos M, Pensler JM. Breast Augmentation. PubMed. Published 2021. https://www.ncbi.nlm.nih.gov/books/NBK482206/
- Ramachandran K. Breast augmentation. Indian Journal of Plastic Surgery : Official Publication of the Association of Plastic Surgeons of India. 2008;41(Suppl):S41-S47. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2825138/
- Perry D, Frame J. The history and development of breast implants. The Annals of The Royal College of Surgeons of England. 2020;102(7):478-482. doi:https://doi.org/10.1308/rcsann.2020.0003
- Kazankaya F, Ahsun Paker S, Demirel Bozkurt Ö. Breastfeeding After Breast Augmentation Surgery: A Scoping Review. Florence Nightingale Journal of Nursing. 2024;32(1):99-109. doi:https://doi.org/10.5152/FNJN.2024.23231