





Elegant Precision™ Rhinoplasty
Contents
- 1 Chapter 2: Rhinoplasty: Introduction
- 2 Chapter 3: Why Are People Afraid?
- 3 Chapter 4: Rhinoplasty Types
- 4 Chapter 5: Candidates
- 5 Chapter 6: Goals
- 6 Chapter 7: Special Cases
- 7 Chapter 8: Revision Surgery
- 8 Chapter 9: Rhinoplasty: Procedure
- 9 Chapter 10: Septoplasty & Turbinoplasty
- 10 Chapter 11: Anatomy
- 11 Chapters 12 & 13: Candidate Pictures & Before/After
- 12 Chapter 14 & 15: Anatomy & Nasal Diagram
- 13 Chapter 16: CAT Scan
Chapter 2: Rhinoplasty: Introduction
[0:00] (Gentle music) Dr. White: Hi, I’m Dr. White. Thank you for taking the time today to learn more about rhinoplasty. Rhinoplasty is also called nasal or nose reshaping, and more commonly called a nose job. It’s considered the most difficult of all plastic surgery procedures, and it’s also my favorite.
[0:23] This is why I actually chose to do ear, nose, and throat (otolaryngology) training, and become fully certified as an ENT doctor before I went into plastic surgery—because I wanted to be the expert on the face before I learned all of the body procedures. The reason rhinoplasty is considered the most difficult of all plastic surgery procedures is really because, first of all, it’s in the middle of your face. And if it doesn’t turn out the way that you’d like, you really can’t cover it up.
[0:55] Second, it’s a game of millimeters. If you change one thing, very often, everything else changes as well. And so, each aspect of the nose is related to another aspect. It’s similar to the law of unintended consequences. So you have to be careful to consider the other features, not only of the nose, but also the face.
[1:18] Third, there’s some degree of unpredictability regarding the nose. The nose is made of bone, cartilage, and skin. Each of those components can heal to a variable degree and it can be somewhat unpredictable. So that’s why rhinoplasty is considered the most difficult of all plastic surgery procedures, but it’s also my favorite. So I’m so happy that you’re here today to learn more about rhinoplasty.
Chapter 3: Why Are People Afraid?
[1:44] (Gentle music) Dr. White: So why are so many people afraid of rhinoplasty? I mean, some people are just scared of having a rhinoplasty done. Well, I think the reason is we’ve all seen a bad nose job. And part of that has to do with how the operation is performed, how it was done in the past, but also the commitment of the surgeons who do the operation. It’s the hardest operation of all.
[2:14] One of the reasons it’s so difficult is it’s kind of hard to teach rhinoplasty. You’re working in a very small area. If the senior surgeon is operating, often, they’ll move their head to the side, and they’ll say, “Do you see this?” And the younger surgeon goes, “See what?” And then they say, “Well, no, here, look again. Do you see it now?” Very often he goes, “Uh-huh, uh-huh,” when in actuality he really never understood what was going on.
[2:42] That’s one of the reasons why ENT surgery is such great training for rhinoplasty. After so many years of doing trauma in eight years of residency, I worked in three county hospitals and very frequently was on call every third night for facial trauma. You see patients with gunshot wounds, shotgun wounds, and trauma with pieces everywhere. You get to know how to put Humpty Dumpty back together again. It gains an appreciation of understanding not only how the nose should look, but also how it should work. That relates to working on the inside of the nose and understanding the sinuses, the septum, and the turbinates.
[3:56] Why then are so many people afraid of rhinoplasty? If you’ve been to a few parties, you’ve seen someone and said, “Wow, I mean that’s just way overdone. I don’t wanna look like that.” Part of the reason for that is some of the older rhinoplasty techniques involved reducing tissue. The surgeon would go in, remove a fair amount of tissue, sculpt the nose, and say, “Voila, this is great.” The problem is the nose continues to change over time. If you take a larger nose and make it smaller, you haven’t really done anything to the skin. The skin on the top will then shrink to fit the smaller nose, and very commonly, the contractile force of that skin will tend to collapse that nose. That’s what leads to a lot of problems over time.
Chapter 4: Rhinoplasty Types
[5:19] (Gentle music) Dr. White: I’d like to explain the difference between an open versus a closed rhinoplasty. Some people would call this an endonasal versus an external approach. The concept is, are you working on the nose just from the inside, or are you actually making an incision, lifting the skin up in order to reveal the nose and to really see all the different parts?
[5:51] The older approach very commonly is the closed approach. The surgeon would make a few small incisions on the inside, reach around, remove some cartilage, take down a hump, close it up, and say, “Wow, I’m done.” It’s a very quick procedure. However, it tends to be very unpredictable. As you open it and flip the cartilages around, you distort the nose.
[6:29] I think the easiest analogy would be this: If you’re working on the engine of your car, lifting the hood slightly, putting your fingers in, and feeling around is essentially what a closed rhinoplasty is. An open rhinoplasty is lifting up the hood, putting your head in there, and seeing what you’re doing. Obviously, you’re gonna do a better job if you can actually see what you’re doing. The open rhinoplasty involves a very small incision right across the columella, and the rest of the incisions are tucked up under the wing or the ala of the nose. I have yet to have a patient ever complain about the columella incision.
[8:09] The approach that I prefer is open structure rhinoplasty. I will open the nose, lift up the skin, inspect the tissues, determine the deformities, determine what tissues are available, and then make a series of sequential changes in order to obtain the most naturally balanced nose for each individual’s face. Often I take pieces of cartilage—your own cartilage ideally—and carve that into small pieces to provide different support beams.
Chapter 5: Candidates
[9:33] (Gentle music) Dr. White: Candidates for rhinoplasty are patients who are healthy, without significant underlying medical problems, who are non-smokers and not using nicotine in any form. Nicotine can squeeze the blood vessels and lead to a healing problem, which is why patients are instructed to stop all nicotine for one month before and one month after surgery.
[10:05] We also want to look for any other ENT pathology such as sleep apnea, nasal polyps, or significant sinus disease, in addition to analyzing the inside of the nose. Very frequently, patients have significant nasal airway obstruction and allergies (allergic rhinitis). We also consider the history regarding any possible nasal trauma or acquired deformities, and consider how well the nose works.
[11:00] Patients frequently will complain that the nose is a little big, that there’s a hump, or that the tip is asymmetric or crooked. We want to do a very thorough nasal analysis. As a general rule, we consider the size, the shape (is there a dorsal hump or a scooped saddle nose deformity?), the length, the tip projection (how far the tip pokes out), and the rotation (is it too high or drooping?). Another consideration is the alignment.
[12:43] If we look from below, we wanna consider the nostrils. Are they asymmetric? What about the ratio of the nostrils to the infratip lobule? Often, we prefer about a two-to-one ratio. So there are a lot of considerations regarding not only the size of the nose but also the shape of the nose, both inside and outside.
Chapter 6: Goals
[13:22] (Gentle music) Dr. White: My goal is to create a natural-appearing nose, which is in balance with your other facial features. We want a nose which not only looks good, but also works well.
[14:20] After surgery, there’s a potential for asymmetries or possibly alignment issues. So those are things we wanna pay special attention to at the time of surgery. My job is to teach you how the nose interrelates and help you understand the anatomy. If you change one thing, everything else may need to change in some way as it relates to that.
[14:59] It’s been said that there’s no such thing as a perfect nose. If your goal is perfection, it is probably best not to have surgery. The revision rate among rhinoplasty surgeons is approximately 15% in the US, which is actually quite high. That underscores not only the difficulty of the operation, but to some degree what the patient’s expectations may be. For example, someone who has very thick skin is never gonna have a very thin, sculpted nose because the tissue over the top will not accommodate that.
[16:21] When we break the bones during rhinoplasty, we don’t fixate it in place with plates and screws. We align it, put a splint on the outside, cross our fingers, and say, “Okay, this is where we want it to heal.” Hopefully it does, but it is possible that it could move a bit. The cartilages also have some degree of memory.
[17:25] Regarding revision surgery, my policy has been that after everything is healed—we wait about two years because the nose continues to change—if there is a change that could be improved upon, the cost would be the normal anesthesia and OR, and my fee would be at half off. I’m committed to doing whatever it takes at the time of the initial operation to get the best possible result for you. Fortunately, my revision rate is much lower than 15%.
Chapter 7: Special Cases
[18:40] (Gentle music) Dr. White: I want you to understand the difference between the reduction of a nasal fracture and a true rhinoplasty. If a patient gets hit in the nose hard enough to break the bones, the skin’s blood supply has been compromised. If the surgeon were to do a true rhinoplasty right after, there’s a reasonable chance the skin may not survive. So in the face of an acute trauma, we typically wait about six weeks to let the swelling go down and the skin recover. All we’re doing in those early fracture settings is realigning the bones to get them back to where they started.
[20:30] I wanna introduce you to the term “tension nose.” It’s associated with a growth of the nose outwards instead of being wide. Frequently, when they look straight on in the mirror, they’re very happy. However, when they turn to the side view, very often they have a hump or the tip comes out too far (increased projection). Essentially, we take the big nose, make it proportionally smaller, build the structure back into the nose, and then redrape the skin over the top.
[22:07] I like to think of it as a puffy nose. Much like a tent, if you have a large tent, reconfigure it into a smaller tent, and put the same big tarp on top of it, that big skin has to shrink to fit the smaller one. Early on, there’s swelling, and as it shrinks, you’d better hope that you built support into the nose, otherwise it will tend to collapse over time. That shrinkage process is individual; it can take months, or sometimes three to four years. You have to be patient.
Chapter 8: Revision Surgery
[24:11] (Gentle music) Dr. White: Rhinoplasty revisions are fortunately less common today than they were in the past because of the open structure approach. What type of support are we discussing? Cartilage tends to give the best support. It’s best to use your own tissues because if you use tissues from someone else (like a cadaver rib), there is some degree of a mismatch and your body may reject or resorb it over time.
[26:02] The septum has cartilage which works very well, provided there’s enough. If someone has had a septoplasty before and that tissue has been discarded, we may need to find tissue from somewhere else, most commonly the rib. Ear cartilage is of limited amount and the quality is perhaps not as good for structural support. A rib graft involves a small incision underneath the breast, taking a piece of the cartilage, carving it into multiple pieces, and building the structure back into the nose.
[26:59] Revision nasal surgery can be very complicated mainly because the tissues have been changed in some way. You don’t really know what you have until you get in there. You have to open things through previous scar tissue, analyze what you have, figure out what you need, make the changes, and build the support back in.
Chapter 9: Rhinoplasty: Procedure
[28:02] (Gentle music) Dr. White: On the day of your surgery, we’ll meet and then we’ll go back to the operating room. The anesthesiologist will put you to sleep. The procedure takes however long it takes to get the best result for you. I lift up the tissues, look at the lower cartilages, the upper cartilages, and the nasal bones. Very frequently, we take the nose apart, work on the bones and cartilage, and reposition it.
[29:16] At the same time, we’ll address the inside of the nose if the septum is crooked, and if the turbinates are enlarged. After we’re done, we’ll have a splint along the outside. We also use splints on the inside to hold the septum and turbinates apart to allow better healing. After the splints come out (usually a week to 10 days), you have to use nasal saline to keep things moist.
[30:07] Early on, expect some degree of swelling and bruising, particularly in the cheeks and eyes if the nasal bones are broken. Expect some bleeding for a day or so. When we take the splint off on the outside, the nose will begin to swell, but as it goes down, the nose tends to look quite good right away. If you like it early, you tend to love it late.
[31:44] As it heals, keep an eye on the alignment. It is possible that it could drift from side to side. I had a patient who slept on her side, and her nose started to drift toward that side because of the weight of the tissue. I told her to sleep on her back or the other side, and sure enough, it went right back to the center. So minimize the risk of trauma after surgery.
Chapter 10: Septoplasty & Turbinoplasty
[33:52] (Gentle music) Dr. White: Now I’d like to explain the anatomy of the nose. The septum divides the nose into two parts. The outside of the nose is composed of a bone, the upper lateral cartilage, and the lower lateral cartilage, which forms the tip defining point.
[36:03] If we look at the nose from the inside, as we go further back beyond the nostrils, we have the superior, middle, and inferior turbinates. A turbinate is a bone covered with erectile tissue, and the lower one is the big one. In patients with allergies, it may be quite big. If we straighten the septum, that improves breathing, but does nothing for allergies. If we make the inferior turbinates smaller, there’s more room to breathe, plus that’s the tissue that causes allergy symptoms, so it can sometimes cure the allergies.
[38:45] The way I have found works best is to do a submucous resection of the turbinate. I lift up the tissue, remove the excess tissue, and roll it up such that the bone is smaller. We use a sterile plastic splint on the inside to keep it from forming a scar band. Don’t use nasal packing (gauze up your nose)—that’s a horrible thing. This is a silastic piece of plastic that slides right out.
[40:06] (Dr. White reviews internal nasal diagrams and photographs of removed turbinate tissue, demonstrating the significant size reduction possible and sharing patient success stories regarding cured allergies and vastly improved breathing.)
Chapter 11: Anatomy
[55:34] (Gentle music) Dr. White: I wanna demonstrate the tent concept for rhinoplasty. (Dr. White uses a board model) The board in the center demonstrates the septum. The nasal bone is up high, then the upper lateral, and the lower lateral.
[56:45] When we talk about grafts, a dorsal spreader graft goes along the dorsum. A lateral crural strut graft (or alar batten graft) runs along the side wall, and the columellar strut runs up the middle. This provides a tripod of support for the tip. The narrower the nose, the more significant impact the septoplasty and turbinoplasty may have on the improvement of the patient’s breathing and allergies.
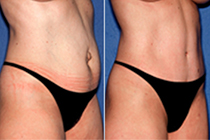
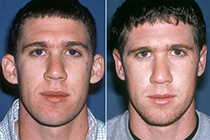
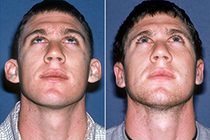
Chapters 12 & 13: Candidate Pictures & Before/After
[58:28] (Gentle music) Dr. White: As we consider the best candidates for rhinoplasty, we consider: Is the nose too big? Is it too long? Is there a hump? Is the tip projection increased?
(Dr. White reviews extensive before-and-after photographs of various patients, highlighting specific corrections such as “boxy tips,” “tension noses,” “dorsal humps,” and cases where internal septoplasty/turbinoplasty was combined with external refinement to improve both aesthetics and breathing function. He emphasizes that reshaping the nose often softens the face and allows the patient’s other features, like their eyes and lips, to pop.)
Chapter 14 & 15: Anatomy & Nasal Diagram
[1:25:12] (Gentle music) Dr. White: So Jennifer’s been kind enough to allow me to demonstrate the nasal anatomy. The glabella is the area between the brows. The radix is the nasal starting point. The bridge is the dorsum. The rhinion is the term where the nasal bone stops and the cartilages begin.
[1:36:00] One thing most patients are unaware of is that there is no cartilage out here at the end of the alar rim (the nostril base). It’s only skin, much like an earlobe. If a patient feels they are wide across the base of the nose, it can be brought in, but we have a trade-off of placing a scar that might potentially be visible.
(Dr. White reviews detailed anatomical diagrams from lateral, frontal, and basal views to visually reinforce the structural components of the nose and the surgical techniques discussed earlier, such as cephalic trims and spreader grafts.)
Chapter 16: CAT Scan
[1:47:53] (Gentle music) Dr. White: Now, I’d like to share with you some CAT scan images of the inside of the nose with a special attention on the septum as well as the turbinates. The bone shows up in white, the soft tissue shows up in a lighter color, and the black shows up as air.
[1:49:14] You can see that the nasal airway is very narrow in these patients. You see this very large soft tissue with a little bit of bone within it—that’s the inferior turbinate. All of this soft tissue is what makes those secretions that get us itchy, sneezy, watery noses. It’s striking to me how many surgeons only operate on the septum. If you only straighten the center but leave these two huge turbinates alone, you only get some improvement. Opening this up can make a huge difference in breathing and sometimes take care of snoring.
[1:59:16] Let me go a little further. Okay, I’ll make it quick. Cameraman: Keep rolling, keep rolling. Dr. White: So this is another example of a CAT scan coronal further back where you can see how big her inferior turbinates are and how much they obstruct her nasal airway…